Hi all,
Today we have a guest post from Dr. David Lendrum, an ER physician at the Foothills Hospital in Calgary. Dave is a super brilliant doc, and this post will outline how to perform BIPAP using a ventilator, as opposed to bringing an extra BIPAP machine into an already crowded resus area. This is particularly useful for delayed sequence intubation (DSI) or prior to intubating the severe metabolic acidosis patient.
These two concepts have been discussed by EM critical care guru Scott Weingart in the podcasts linked below. If you haven’t heard them, stop reading and go listen now.
Intubating a patient with severe acidosis
Delayed Sequence Intubation
This post is to demonstrate how to actually accomplish this using our ventilators, and thus may be more useful for the local Calgary docs than others. However, the steps should be applicable to most ventilators. I also look forward to feedback regarding better, faster, easier ways to do this.
The post contains text and photos, with a video at the end. You can also link to my other “How To” videos here.
On with the post.
1) To “BIPAP” a patient we are basically talking about providing a patient with an amount of pressure support when they inspire and an amount of PEEP when they exhale. We almost always ask the RT’s to bring a “BIPAP” machine to the bedside as we don’t seem to use the actual ventilator to do this. Why is this??? Mainly because these machines do BIPAP really well, the are simple to use and they are also portable, meaning they can be hooked up to an bottle of oxygen and the patient can be transported while being BIPAP’ed where as this can’t be done with the large ventilators. The downside is that they are really large and take up a lot of real-estate in the trauma bays and such.
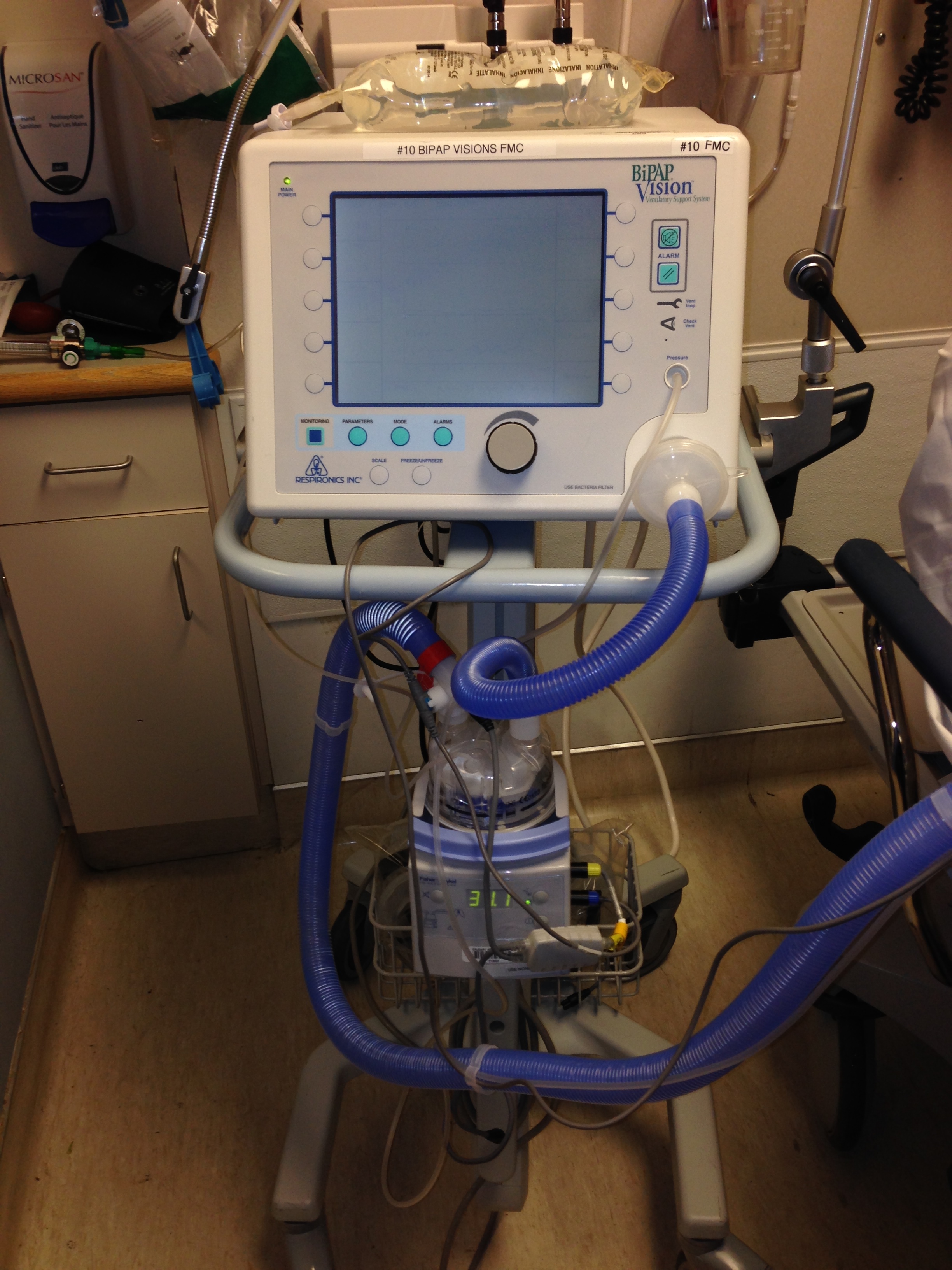
FMC BIPAP MACHINE
2) You may not know that you need to use a special mask with the BIPAP machine! I don’t mean that it is special in the fact that it is nice and soft and needs to be on the patient really tightly, but there are actually two different masks for non-invasive ventilation.
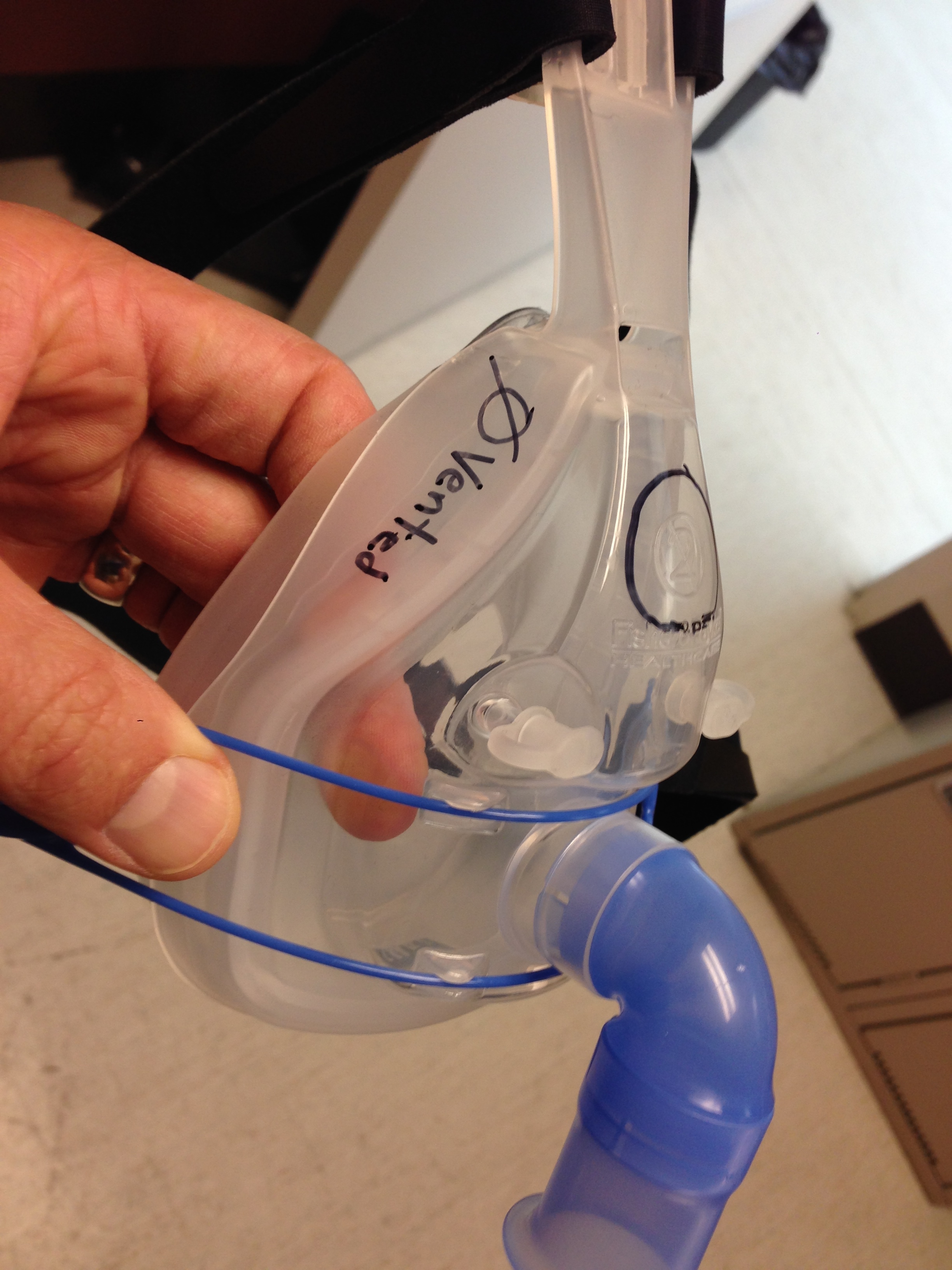
BIPAP MACHINE: As you can see there is only one tube going to the patient providing air, but no return circuit. As such, where does the patient exhale? You MUST use a mask with exhalation holes in it with this mask or the patient can’t exhale at all other than leaking around the mask. The photo below shows the mask the RT’s will put on the patient which has these holes or vents.

3) You most definitely can do non-invasive ventilation with the regular ventilators we have in the department. However, you need to use a special NON-VENTED mask as the ventilator DOES have a exhalation tube that returns to the machine. As you can see, the NON-VENTED mask has the blue nose looking thing and no holes in it.
4) Bringing a BIPAP machine into a code room when I have every intention of intubating them in the near future makes no sense. The RT’s agree with me. As such, I have done some playing with the vent and figured out ONE of the ways of doing this. I am sure some of you will have lots of comments on other ways of doing this as well.
5) Find a ventilator and let the RT know what you are thinking. “I want to non-invasively ventilate this patient until I am ready to pass the ETT”. Perhaps you are doing this for a patient with an ASA overdose or a severe DKA patient and you are really worried that if the patient becomes any more hypercarbic they really aren’t going to do well. Or, maybe they are wild and crazy and have a severe pneumonia and you feel that they need some sedation and pre-oxygenation prior to intubation.
6) Here is what the ventilator looks like in standby mode.

7) You can attach the ventilator hosing to the the NON-VENTED BIPAP mask if you wish. Notice I have also hooked up the end-tidal CO2 to this set up which would be helpful as well. If you can’t find the non-vented mask you could use the vented one, but there is just going to be a big “leak” out the holes. It wouldn’t be dangerous, whereas doing the opposite (using a non-vented mask on the BIPAP machine would be).

8) I also like this set up as it totally removes any concern of using a special mask and would solve the same problem, but just require someone to maintain a good seal with the patient. I suspect to do this well you would have to have a obtunded or very cooperative patient. This is where some Ketamine/Haldol might go a long way.

Here’s a video showing the process.
Agree/disagree? I look forward to your comments. Post them here, or tweet @socmobem.
Dave Lendrum
Leave a Reply